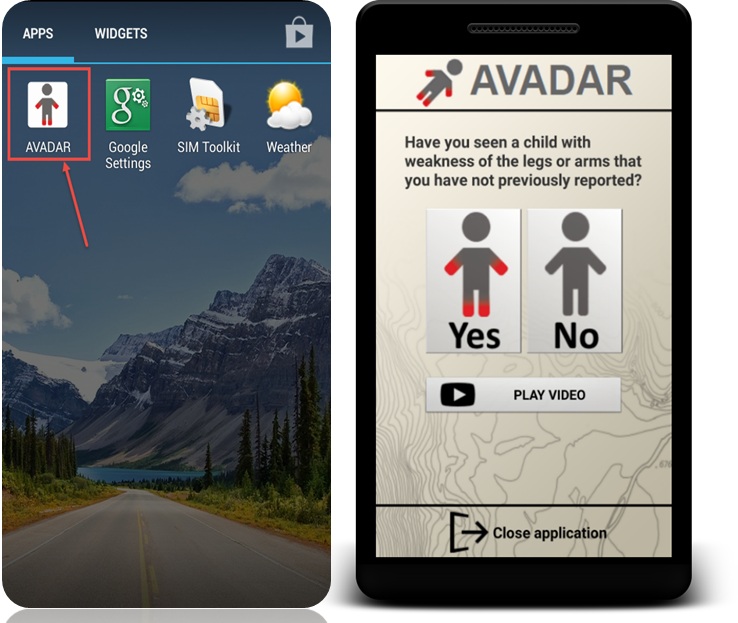
Auto-Visual AFP Detection and Reporting (AVADAR) is a mobile sms-based software application designed to improve the quality and sensitivity of Acute Flaccid Paralysis (AFP) surveillance by health workers and key informants within hospital facilities and local communities.
countries
Burkina Faso, Cameroon, Central African Republic, Chad, the Democratic Republic of Congo, Liberia, Mali, Niger, Nigeria, Sierra Leone, South Sudan
funding
Bill & Melinda Gates Foundation
Auto-Visual AFP Detection and Reporting (AVADAR) is a multi-country project currently operational in 11 polio high-risk countries in Africa: Burkina Faso, Cameroon, Central African Republic, Chad, the Democratic Republic of Congo, Liberia, Mali, Niger, Nigeria, Sierra Leone, and South Sudan. eHealth Africa has provided downstream technology support in eight of these countries and continues to support ground operations in two countries, while providing equipment support in six of these countries.
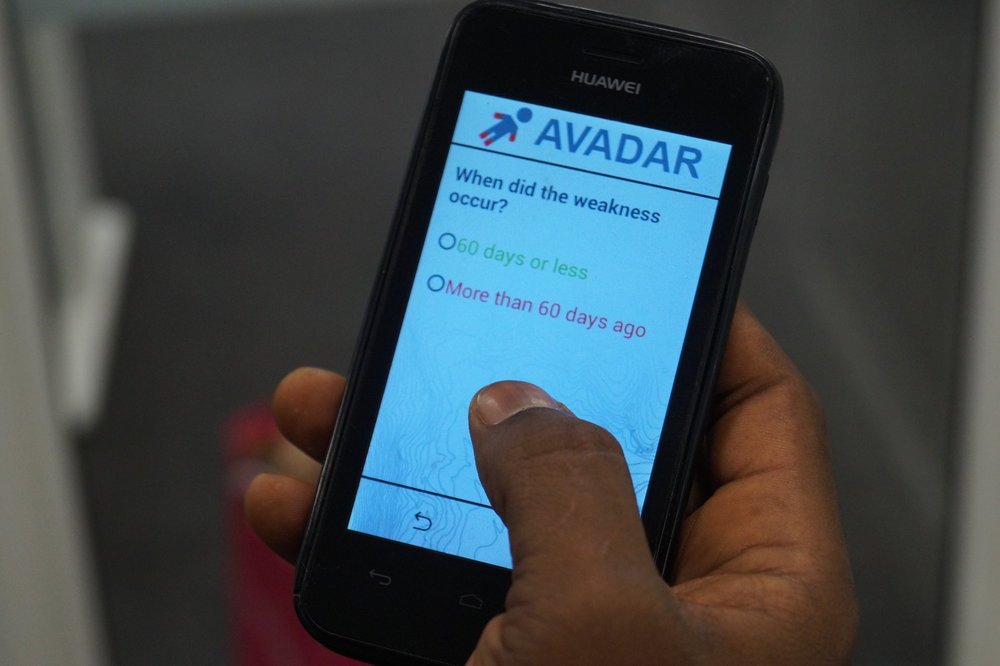
Acute Flaccid Paralysis (AFP) is the main indicator of polio. AVADAR improves the traditional AFP surveillance systems by “widening the net” of disease reporters and using an sms-based mobile technology to improve the completeness, timeliness, and availability of AFP reporting. When informants report suspected AFP cases, automatic case alerts are sent to the appropriate disease surveillance officers who go to investigate, while the resulting data is automatically aggregated, visualized, and made available for decision makers.
AVADAR is an important component in the global “end game” for polio.

eHA's role
Customize AFP video into local languages
Customize trainings for informants based on country / local context
Train informants in local languages using locally-recruited facilitators
Resolve weekly technical issues in the field for informants
Assess and negotiate telecommunications network contracts for informants
Procure and ship equipment based on country import regulations
Stakeholder Collaboration
Planning, implementation, and monitoring of the AVADAR project is a collaborative effort between government stakeholders in each country and program partners. Three key areas of collaboration are:


Mobile Application
The AFP video component was developed by World Health Organization (WHO) and eHA, and the software design component was handled by Novel-T. To date, eHA has translated the app into 17 languages.
Informant Selection & Capacity Building
The selection of informants (including health workers) was led by the WHO and each country’s Ministry of Health team. Once selected, screening and training was jointly conducted by WHO, the Ministries of Health, and eHealth Africa team.
In several countries, “special informants” with limited literacy participate in the project via a simplified version of the app that only requires a “yes” or “no” response to having seen a child with AFP symptoms. There are currently 156 special informants in the AVADAR network of 5,198 trained individuals.
Field Monitoring & Supervision
Joint supervisory field visits are conducted on a monthly basis by WHO, Ministries, and eHealth Africa field teams to provide troubleshooting phone support for informants, conduct re-training sessions, and identify noncompliant informants. eHA has resolved 8,467 technical phone issues.
Provision of AVADAR equipment
Informants, investigators and district coordinators need mobile phones to consistently send their reports. Those in remote areas also need power-banks with solar chargers to ensure they remain on the network and send in their case reports every Monday. Investigators need ODK enabled mobile phones to effectively investigate reported cases. Since 2016 to date, eHA has supplied the complement of mobile phones, batteries, USB cables and solar chargers needed to sustain the project. In 2020, we will be providing further equipment support to six countries.
Sustainability
To ensure the longevity of the project and its efficiency, eHA has been transferring most of its responsibilities to the relevant ministries of health and the World Health Organisation. Thus, the transition program is a phase of training and capacity building to equip actors with the skills they need to handle the work we do effectively and prune down on the running costs of the project. To ensure the effectiveness of the transition efforts in 2019, eHA trained a total of 501 persons including; 217 first level support persons, 53 second level support persons and 233 new Informants (in Liberia and Sierra Leone only), to continue to support the project in six countries namely, Chad, DRC, South Sudan, Cameroon and Niger.
Training and Capacity Building
Our transition efforts also include equipment transfer to WHO and Ministries of Health. Successful transitions will ensure that surveillance systems are strengthened in all target countries in the foreseeable future. So far, eHA has transited operations in six countries; Chad, the Democratic Republic of Congo, Liberia, Nigeria, Sierra Leone and South Sudan, and still maintains operations support in two countries; Cameroon and Niger Republic. At the end of transition in 2019, eHA transferred to WHO; 1,413 phones, 912 solar chargers and 213 phone batteries.
beneficiaries
National and state governments across Burkina Faso, Cameroon, Central African Republic, Chad, the Democratic Republic of Congo, Liberia, Mali, Niger, Nigeria, Sierra Leone, and South Sudan
Local communities across Burkina Faso, Cameroon, Central African Republic, Chad, the Democratic Republic of Congo, Liberia, Mali, Niger, Nigeria, Sierra Leone, and South Sudan
Impact
6,746
Community informants trained in eight countries
68,982
suspected AFP alerts investigated by Disease Surveillance Officers
3,710
confirmed true AFP cases
5,591,753
people being observed for AFP in six countries
29,117
suspected AFP cases reported in 2019
783
hours spent on capacity building activities to strengthen AFP surveillance and reporting systems in six countries
Success Story


Read more