Although the Democratic Republic of Congo (DRC) has been polio-free for more than 20 years, it is still considered a polio high-risk country by the World Health Organization. The recent recurring Ebola Virus disease outbreak has shown just how vulnerable the DRC can be to infectious diseases. Dr. Blaise Kalenga is the Chief Medical Officer of the Haut-Katanga region, one of the 26 provinces in DRC. He coordinates and monitors all the AFP surveillance activities conducted within the region including notification, investigation, confirmation, and reporting of cases. Several factors contributed to make AFP surveillance an arduous task in his province and in the country as a whole. One of these factors was the dependence on the traditional surveillance methods which had proved ineffective. In addition, covering DRC’s large land area was very difficult. A large proportion of DRC’s population is scattered across the landmass and some of the population reside in very hard-to-reach localities. Insecurity in several rural areas was also significant, causing massive migration or displacement out of target locations, to safer areas. This weakened the routine vaccination system and hampered the active search for AFP cases or tracking of potential carriers.
“AFP surveillance was particularly difficult due to the insufficiency of data management and surveillance tools—standard case definition documents, AFP posters, surveillance guidelines—were not available in health centers and health zones. We also faced enormous difficulties in transporting laboratory samples after collection.”
Dr. Kalenga and his colleagues often failed to achieve WHO targets in terms of timeliness and completeness of AFP reporting given the challenges above. These two are important for tracking how frequently suspected cases of AFP are reported, and the proportion of reported AFP cases that are investigated or confirmed by surveillance officers—key indicators which Dr. Kalenga needs for optimal planning and programming in his region.
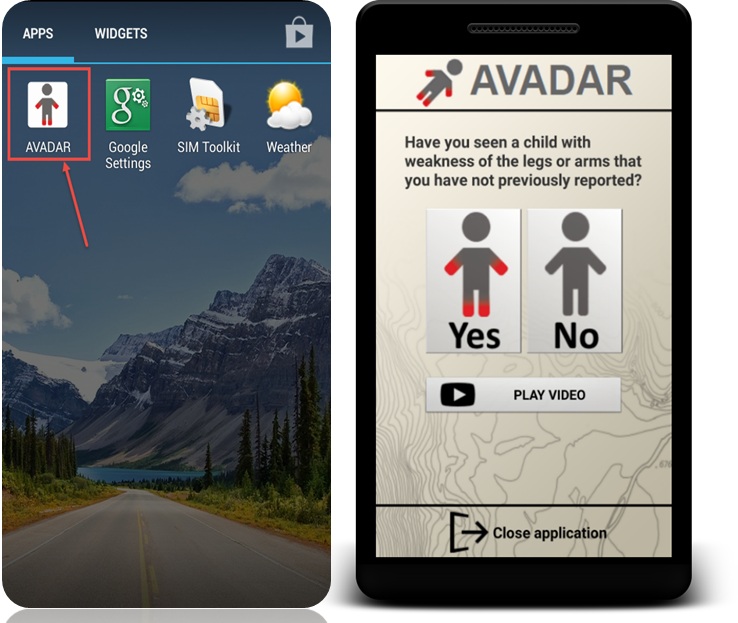
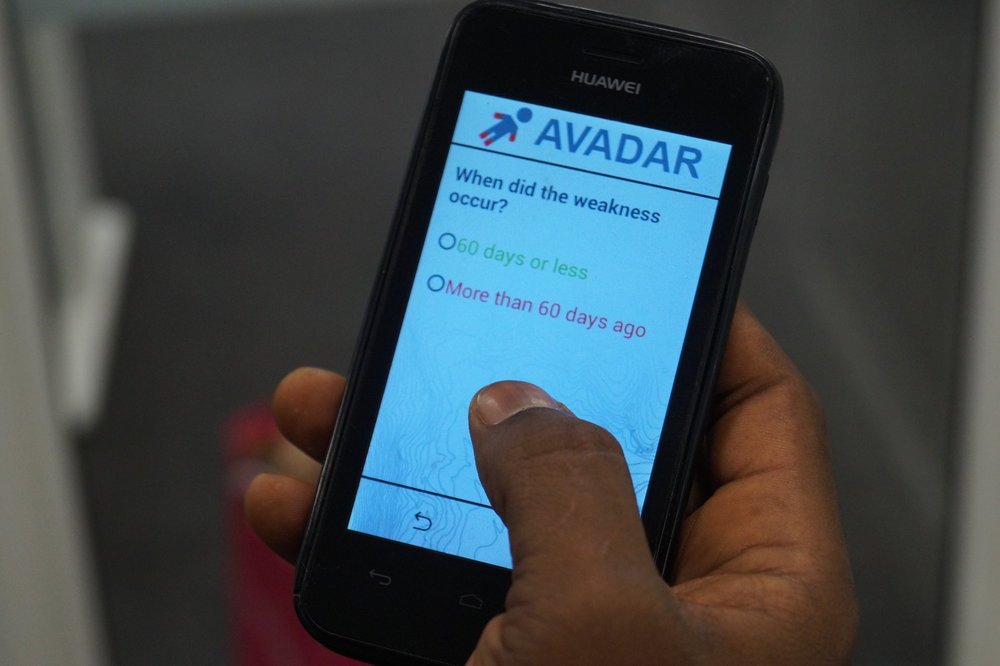
In August 2017, AVADAR debuted in DRC, deploying technology to address the gaps in the traditional, paper-based AFP surveillance system. It decentralized AFP case scouting and made it more inclusive by enlisting more hands from the community, instead of a system limited to identified health workers.
Community-based Informants armed with phones were trained to identify and report suspected AFP cases in the localities where they live. The reports are instantly uploaded onto a server which notifies the surveillance officers via SMS, to conduct further investigations. In a matter of months, AVADAR’s positive effect on AFP surveillance in Haut-Katanga was apparent. Reports of suspected cases increased and a large number now came from previously silent areas. The burden of AFP case finding was no longer solely on the surveillance officers, allowing them more time for investigation. This reduced the turnaround time between reporting and investigation time. An added benefit of the AVADAR program is that the community informants also report cases of other priority vaccine-preventable illnesses and this has strengthened the surveillance system in DRC.
“By providing the community informants with work tools, the AVADAR project has not just improved AFP surveillance in DRC but has improved the standard of living of these informants, who now feel valued. The informants also support the surveillance of other priority diseases and other health activities even without having trained them beforehand.”
Especially beneficial to Dr. Kalenga is that the AVADAR platform allows him to track the activities of all the informants, investigators, and health workers on the platform and to ensure that everyone is delivering on their mandate. In turn, he is better able to address issues as they arise.
“AVADAR has integrated technology into the active search for AFP cases thus providing motivation for health workers to do their jobs better. Investigation and reporting rates in Haut-Kalenga have increased and now we are more confident of our ability to prevent and respond to any outbreaks.”
The DRC has been one of the best-performing countries under the AVADAR project, demonstrating the commitment of its health system to forestall future outbreaks of Polio. In 2018, the DRC AVADAR network averaged a 96% investigation rate in 2018, causing the WHO to sanction an expansion to three new districts in the country last December. With 799 informants, DRC is now the country with the second largest network of informants currently, after Nigeria.
Download this story
Read more