By Daniel Ojabo
In response to the recently reported cases of wild poliovirus in Nigeria, eHealth Africa (eHA) partnered with Bill and Melinda Gates Foundation, WHO, and Novel-T to pilot a mobile-based surveillance application for Acute Flaccid Paralysis (AFP) in children.
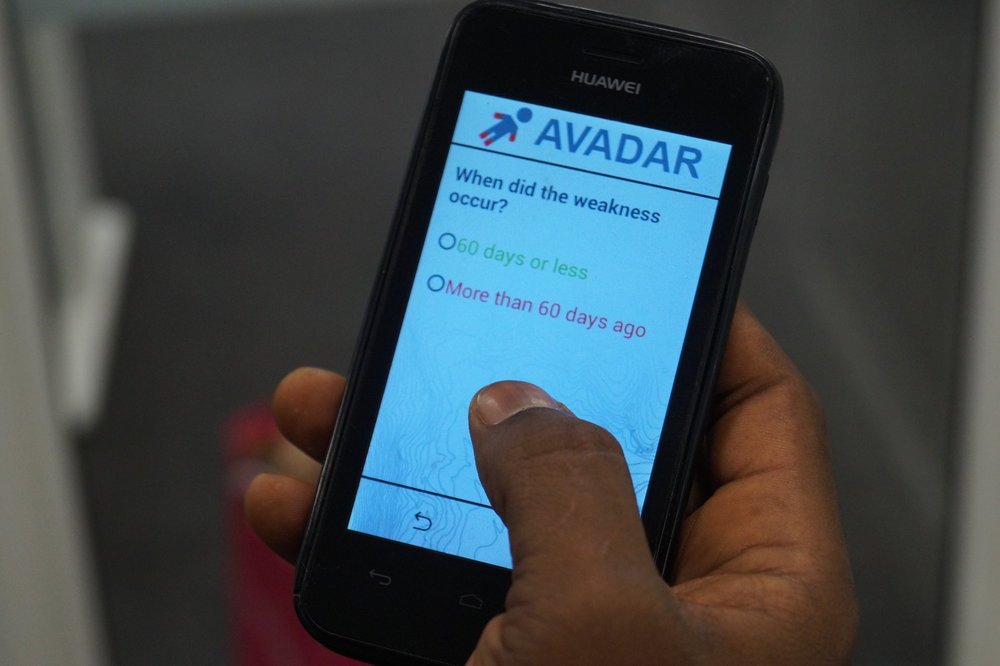
Defined by WHO as “a rapid onset of weakness of an individual's extremities”, AFP often causes weakness of the muscles of respiration and swallowing, progressing to maximum severity within 1-10 days. AFP surveillance, being one of the four cornerstone strategies of polio eradication, seeks to identify all cases of polio through a system that targets any case of AFP as a potential case of polio. The surveillance tool is an Auto-Visual AFP Detection and Reporting (AVADAR) mobile application installed on android-enabled mobile devices, provided to Health Workers and Community Informants, to aid in the detection and reporting of AFP cases within health facilities and local communities.
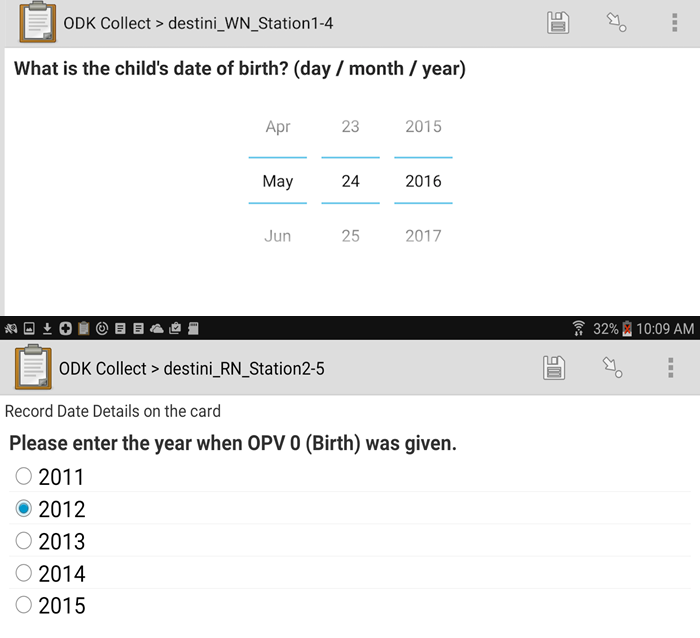
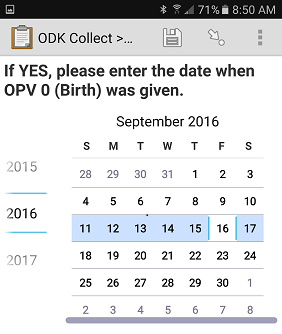
Screenshots of AVADAR Application
According to the project manager, Umar K. Idris, “AVADAR was designed to improve the sensitivity and quality of AFP surveillance, particularly in places with low performance indicators”.
The AVADAR project was piloted on 5 August, 2016 in the Local Government Areas (LGAs) of Oyun (Kwara state) and Kuje (FCT, Abuja) for an 8 week period. In Kuje, community informants reported 26 AFP cases within the 8 week period. This was a considerable increase compared to only 23 cases reported in the 33 week period (from January to July 2016) before implementation of the AVADAR pilot. Similarly, in Oyun there were 8 reported AFP cases within the 8 week period (August to October 2016), compared to only 4 reported cases in the 33 week period prior to AVADAR.
Building on the successes achieved, the project was scaled up to include 8 LGAs in Borno state in November 2016, with plans to further expand into other states.
“We are on the verge of expanding into Adamawa, Sokoto and Yobe. We also aim to implement it in the Lake Chad Region (Chad, Cameroon & Niger Republic), post-Ebola countries (Guinea, Liberia, Sierra Leone), as well as the Democratic Republic of Congo and South Sudan in 2017”, Idris said.
According to the Global Polio Eradication Initiative (GPEI), the absence of AFP surveillance provides a gateway for wild poliovirus to continue circulating around the world. Innovations like AVADAR have already improved the surveillance network by providing health workers and community informants with an active surveillance tool to effectively report suspected AFP cases. The surveillance data will serve as a measure of progress towards polio eradication and allow polio program stakeholders to effectively plan and implement strategies for supplementary immunization activities (e.g. national immunization campaigns).
[youtube=://www.youtube.com/watch?v=EeSzp8H0ODQ&w=854&h=480]
To strengthen communication amongst the local health workers and community informants, eHA trained over 800 health workers and provided them with over 800 GPS-enabled smartphones and solar chargers.AVADAR has expanded the surveillance network by bringing in more community informants, health workers and designated health facilities to improve the sensitivity of AFP surveillance amongst surveillance personnel (in terms of timely detection and reporting). The AVADAR software includes an embedded 30-second video of a live child with AFP symptoms having difficulty crawling/walking, as well as an electronic data collection form for submission of detailed information on suspected AFP case patients. This video is sent as a weekly reminder to Health Workers and Community Informants (on their GPS-enabled mobile phones) responsible for reporting all suspected AFP cases in their health facilities and communities.