By Ayodele Adeyemo & Hawa Kombian
The Cholera Threat
According to the World Health Organization (WHO), cholera (an infectious disease which causes acute watery diarrhea) remains a global threat to public health with an annual average of 82,000 deaths. In Nigeria, the cholera burden has been an average of 10,000 cases annually with over 70% of the cases coming from Bauchi, Yobe, and Zamfara states.
Following the review and recent publication of WHO guidelines on cholera control, the Nigeria Centre for Disease Control (NCDC) has begun the implementation of innovative approaches to tackle cholera via:
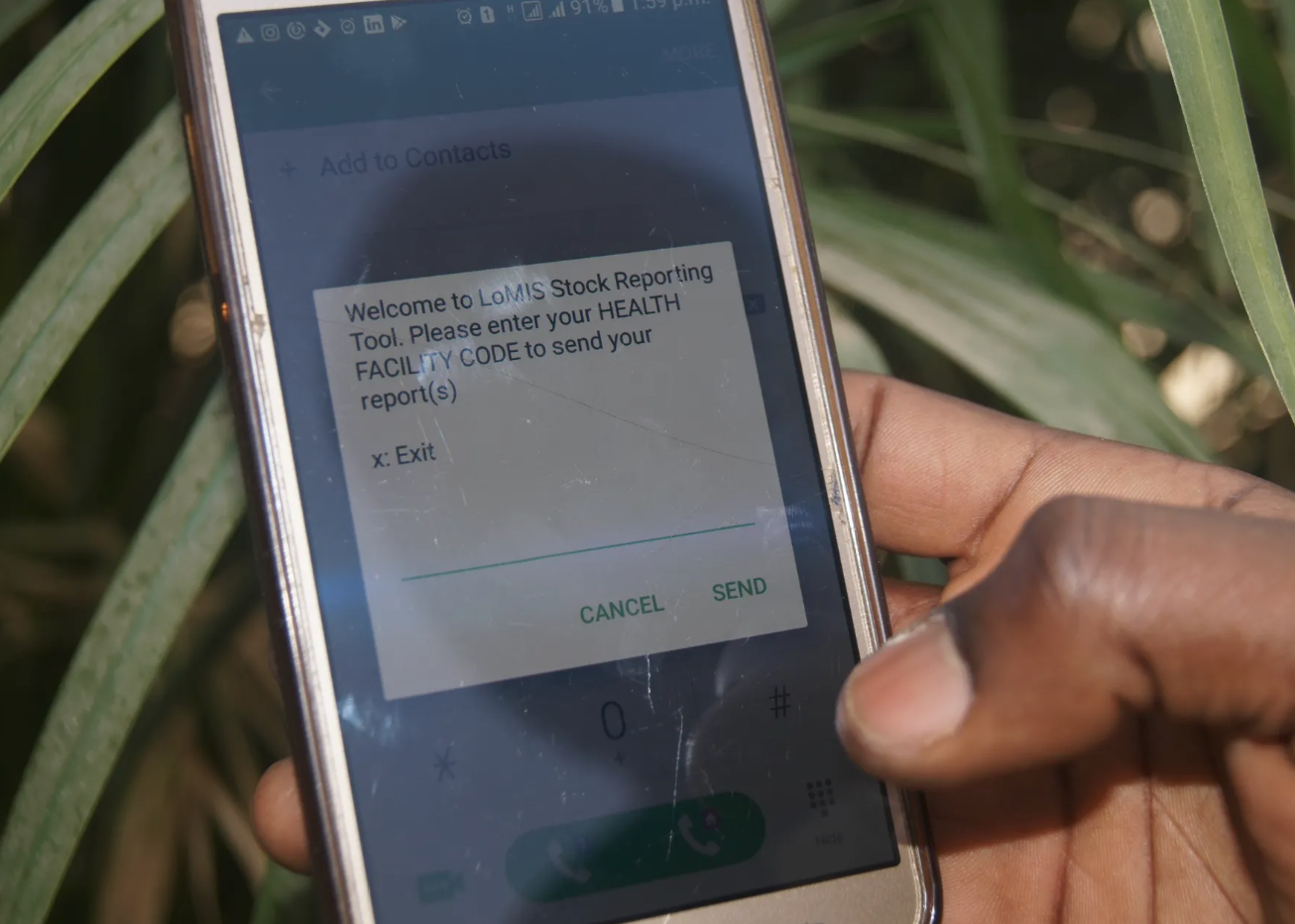
Strengthening disease surveillance for early detection and quick response through innovative use of technology and data.
Improving coordination for technical support, resource mobilization, and partnership.
Adopting a multi-sectoral approach to meet the 2030 cholera elimination by working with the environment and Water and Sanitary Hygiene sectors to ensure that communities have good water and sanitary facilities which will prevent further outbreaks
The Digital Health Advantage
What does an innovative model for cholera prevention and control look like?
In 1854, John Snow mapped out the cholera deaths during an outbreak and observed that they all occurred within short distances and were clustered around the Broad Street pump. He went ahead to carry out statistical tests to illustrate the connection between the source of water and the cholera cases.
In synergistic partnership, NCDC and eHealth Africa (eHA) used advanced geographic information systems (GIS) technologies to build on John Snow’s ideas of mapping. eHA uses data-driven solutions and tools to improve community health, with specific expertise in the design, development, validation, and deployment of predictive models for diseases like cholera.
GIS allow experts to explore different aspects of a geographical point. The identification of patterns can drive insights and enable health stakeholders to make informed decisions about how to best plan public health interventions. Due to computational and technological advancement, GIS has been used in public health for epidemiology, resource planning, and surveillance among others.
NCDC and eHA were able to utilize GIS capabilities to enhance the data management within the NCDC National Incident Coordination Centre (ICC). The ICC serves as a the emergency operations center for coordinating disease outbreaks at the national level.
eHA’s GIS and Data Analytics team works with the NCDC to map cholera hotspots (areas where cholera persists) across Nigeria’s Local Government Areas (LGAs). At the start of the outbreak, hotspot analysis helps determine where to vaccinate and what quantity of vaccines are required per LGA. This exercise ensures the effectiveness of the oral cholera vaccine immunization campaigns which are rolled out to stop the spread of disease.
In planning, data from 2012-17 displays the spread of cholera outbreaks and also shows the relative risks of the various LGAs which have reported an outbreak during the five year period.

The Big Picture Data Source: Nigeria Centre for Disease Control

Data Source: Nigeria Centre for Disease Control
We layered the 2018 outbreak data with the historical hotspot analysis to identify specific trends and possible overlaps. The result of the hotspot analysis identified 83 LGAs as hotspots, with 87% reporting at least one case with over 70% of the burden from Bauchi, Kano, and Zamfara states. The LGAs identified as hotspots have enabled the government to make informed decisions about where to request vaccines to ensure that the most vulnerable areas are supported.
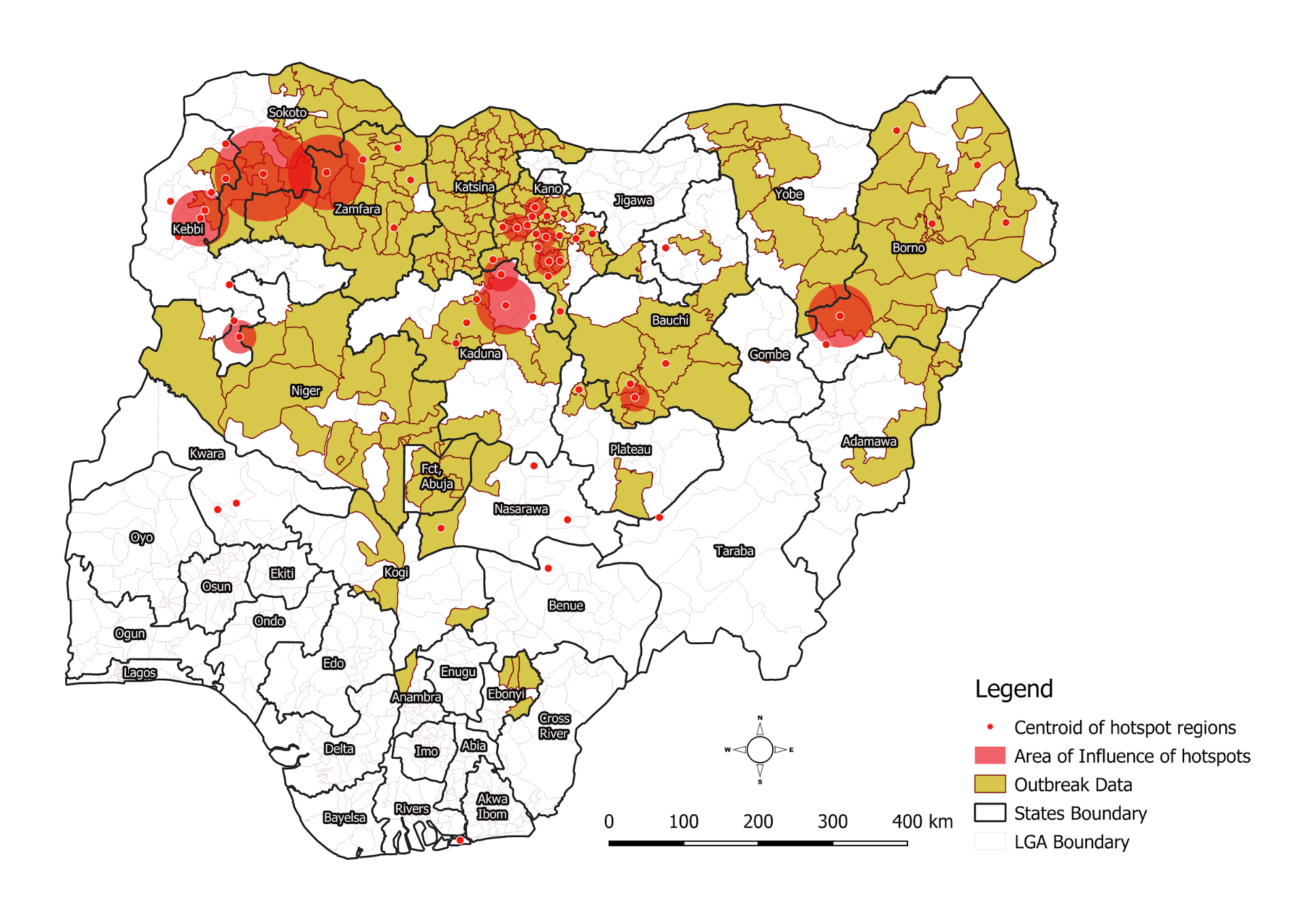
Data Source: Nigeria Centre for Disease Control
We continue to collaborate with the NCDC to strengthen cholera surveillance in Nigeria. The partnership ensures that data management and analysis expertise contribute to faster response and informed decision making before, during and after outbreaks.
This work was done in collaboration with the following partners:
Yennan Sebastian- NCDC
Adesola Ogunleye - NCDC
Heloise Lucaccioni - UNICEF
Helen Adamu - UMB
Kobi Ampah- WHO Geneva