Introduction
In 2020, Nigeria was declared wild polio-free after meeting the requirements to attain the status, which includes 3 years without any new cases of wild poliovirus in the country1. Prior to achieving this milestone, Nigeria was one of only three countries in the wild with endemic wild polio. GIS (Geographic Information System) tracking was first implemented in Nigeria’s Polio program in 2012 with eHA’s Vaccination Tracking project (VTS). VTS was decommissioned in 2020, just after Nigeria was declared Polio free.
Our Intervention
Since 2022, eHA has been providing GIS tracking support to the polio outbreak campaigns in security-compromised locations with the Polio Special Intervention project, which is part of a key focus area of eHA - Public Health Emergency Response Systems. The purpose of this project is to support the efforts to improve the Polio outbreak response in Nigeria, with a focus on circulating variant poliovirus type 2, cVPV2, using the new Geospatial Tracking System (GTS) application to track vaccination teams.
“Special Intervention”, in this context, refers to the security-compromised nature of the implementing states. Due to banditry, kidnapping, and terrorism, several settlements in these states are either inaccessible or partially accessible. Vaccine-eligible children residing in these areas are denied access to their necessary vaccinations such as the Polio vaccine due to the insecurity posed by these activities. Accessing these communities means reaching the missed children and protecting the communities from disease outbreaks and securing a truly polio-free Nigeria. The project is being implemented in 57 local government areas (LGAs) with security-compromised settlements, in 7 priority states- Kaduna, Katsina, Kebbi, Niger, Sokoto, Yobe, and Zamfara.
Geospatial Tracking System (GTS) was introduced by Novel-T after the decommissioning of the VTS application. The GTS application is a “lightweight” version of the VTS and was first piloted in Borno State in 2020 and is currently being used on this Polio Special Intervention project.
The GTS application is used to monitor vaccination teams and report daily missed settlements based on the DIPs (daily implementation plans) of a campaign. The process flow is displayed below:
Results
Since the inception of the project, the eHA-led activity has had a significant impact on the polio campaign implementation. Between September 2022 to May 2023, eHA has supported 66 LGAs with GIS tracking across the 7 implementing states. 3,953 settlements with vaccine-eligible children have been verified to have been visited by the vaccination teams during 2 rounds of polio campaign implementation in the states, using GTS trackers, and 1,664 vaccination teams were tracked during the campaigns.
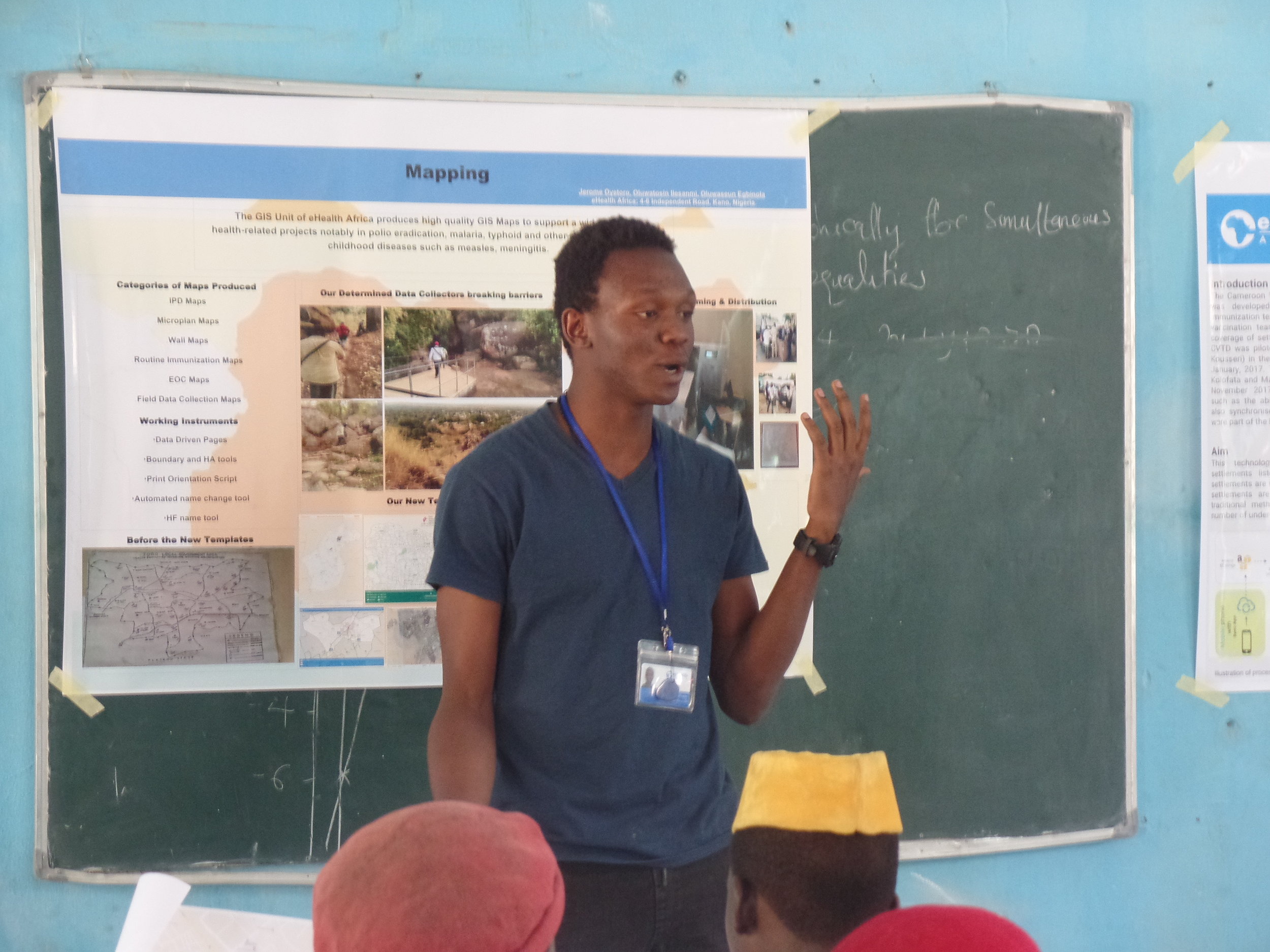
Field technical teams were deployed to each implementing LGA to support the campaign. 66 LGA consultants were trained on the administration and operation of the GTS application. The consultants built the capacity of the LGA team on GIS tracking with trainings on GTS and the handling of the trackers. This was necessary to make sure that the vaccination teams are fully equipped and knowledgeable enough to successfully implement GIS tracking during the campaigns. Data collection activities were also conducted during the campaigns to obtain the geo-coordinates of settlements that are not on the Polio geodatabase (GDB). 69 data collectors were trained on the use of the KoboCollect application to collect geo-coordinate data in the field. This data collection ensured that the visitation of the planned settlements by the vaccination teams could be verified.


Conclusion
GIS tracking has helped increase vaccination coverage throughout the 7 priority states where it was implemented. In addition to increased coverage, GIS tracking also provided data-driven insights for decision-making. It increases the quality of campaign implementation and improves accountability, by validating the tally sheet reports generated by the vaccination teams. GIS tracking can be utilized beyond polio programming to support other vaccination initiatives by improving vaccination coverage and in turn, boosting Nigeria’s immunization indices.
Training of LGA team in Rijau LGA of Niger state on the GTS application and handling of the trackers
Engagement meeting with the Niger State Primary Health Care Development Agency team
L-R : Basheerdeen Abdullahi (eHA State Coordinator), Mohammed Alhaji Usman (State Health Educator), Abubakar Shehu (Program Manager, eHA), Kpantus Abubakar (State Immunization Officer), and Nnenna Ohiaeri (Project Manager, eHA)