According to the World Health Organization, there were an estimated 241 million cases of malaria worldwide, with an estimated 627,000 deaths in 2020, and 80% of these deaths were children under five years from Sub-Saharan Africa.
The populations with the highest malaria mortality tend to reside in hard-to-reach regions of Africa, with limited access to health facilities. Is there something that needs to be in place to reduce the number of malaria deaths? How do we as an organization use innovation and data to reduce the malaria burden and save lives?
Here are three ways we have harnessed innovation to reduce the malaria burden.
Adequate tracking saves lives
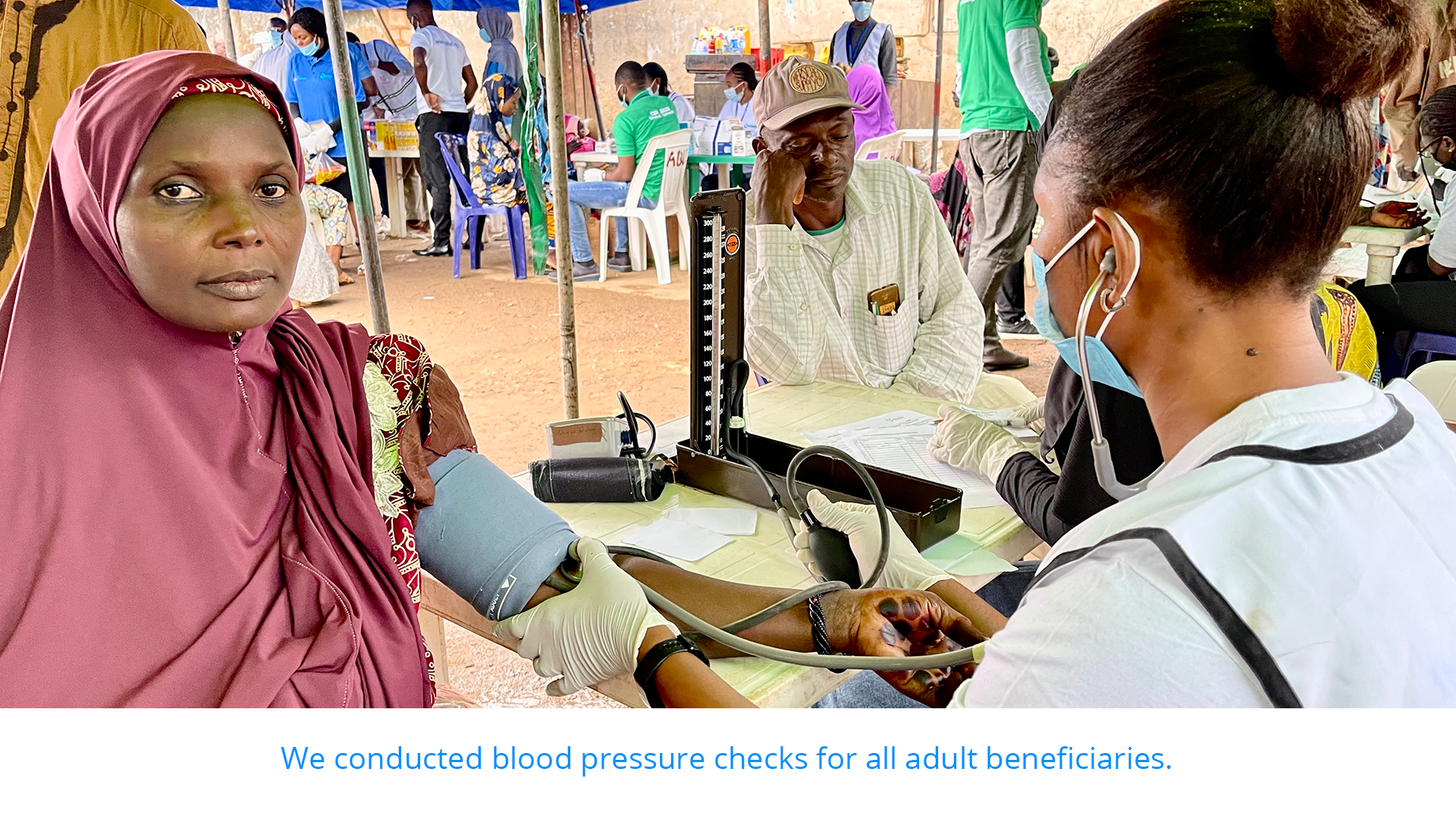
In October 2021, the World Health Organization engaged eHealth Africa to support the Seasonal Malaria Chemoprevention (SMC) Cycle 4 campaign with GIS eTracking across all the 21 Local Government Areas (LGAs) of Adamawa State, and 4 selected LGAs of Yobe State. The campaign was house to house, and we employed the services of Community Drug Distributors (CDD) for drug delivery.
eHA provided technical, equipment, and human resources to support the cycle 4 campaign by collecting and analyzing the passive tracks of the Community Drug Distributor (CDD) teams during SMC Cycle 4 campaign using Vaccinator Tracking System (VTS). We provided VTS for coverage, and this helped with the numbers of houses reached, as the tracker shows any missing location for mop-up. We also tracked the drugs to ensure effective utilization.
Identifying coverage gaps with GIS
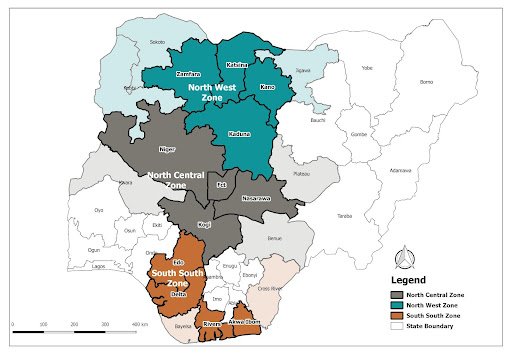
We supported the Malaria Consortium in mapping out nine hard-to-reach local government areas in Kaduna and eleven hard-to-reach local government areas in Kano to make them eligible for ICCM (Integrated Community Case Management). ICCM is a strategy that focuses on training, supporting, and supplying community health workers (CHWs) to provide diagnosis and treatments for illnesses such as malaria, pneumonia, and diarrhea for children of families with difficult access to health facilities. Research has shown that ICCM can potentially decrease the child mortality rate of these three illnesses by a whopping 60%.
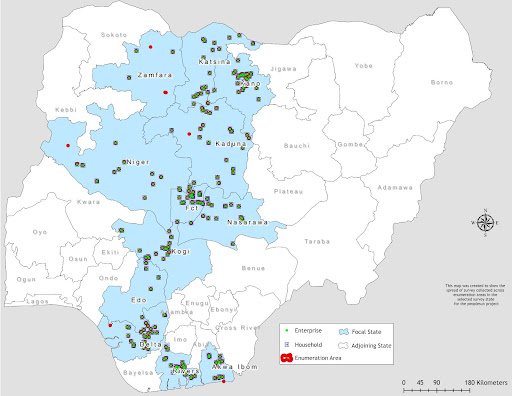
We leveraged our expertise in geographic information systems to collect geospatial data relating to settlement names and locations, and the nearest functional primary and secondary health facilities to the settlements for two weeks.
Access to geospatial data can reduce the malaria burden
We are increasing access to geospatial data in public health planning by opening access to the data we have collected over the years to the public, to allow a wider cross-section of people and organizations access to data that can assist them in decision making and resource planning. We created a tool called the Data Portal, which is a collected catalog of a wide variety of geospatial data and other datasets in the countries and regions eHealth Africa has worked in. We developed this to serve the data access, routine analysis, and informed decision-making needs of government, private sectors, donors, partners, and individuals.
The data is accessible to all for non-commercial use.
With access to this data, the government, non-governmental organizations, relief, and charitable organizations have information on boundaries, settlements, and health facilities; this makes field operations and deployment of resources a lot easier. So when mosquito nets distribution or chemoprevention campaigns are planned, there’s enough data available to serve as a guide, providing information on different settlements and how many health facilities are accessible in those areas.
The fight against malaria is global and still ongoing, and thanks to better prevention and treatment tools, there has been a drop of 44% in the malaria mortality rate in the last two decades in Africa.